Scope and definitions
In 2021, the WHO Expert Committee on Specifications for Pharmaceutical Preparations adopted as an annex to its 55th report the Good reliance practices in the regulation of medical products: high level principles and considerations.
This document defines reliance as ‘The act whereby the regulatory authority in one jurisdiction takes into account and gives significant weight to assessments performed by another regulatory authority or trusted institution, or to any other authoritative information, in reaching its own decision. The relying authority remains independent, responsible and accountable for the decisions taken, even when it relies on the decisions, assessments and information of others’.
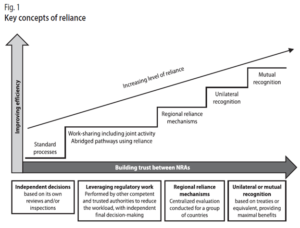
As Figure 1 describes, reliance may take many forms and be applied to varying degrees in recognizing or taking account of the assessments, decisions or other authoritative information of other authorities and institutions. While recognition may be seen as a special and more formalized approach to reliance, whereby one regulatory authority recognizes the decisions of another regulatory authority, system or institution, obviating additional regulatory assessment to reach its own decision. Recognition usually requires formal and binding legal provisions.
Reliance may be used in the regulation of any of the medical products in the scope of SEARN and for all regulatory functions, in the full life cycle of a medical product.
While the precise situations in which reliance may be used are to be defined at the national level, some conditions are required to enable reliance, including having access to sufficient information from the reference NRA such as full/public assessment reports in a common language documenting their regulatory decisions.
Converging on the definition of reference regulatory authorities in SEARN
The WHO Good reliance practices in the regulation of medical products: high level principles and considerations define a reference regulatory authority as a ‘national or regional authority or a trusted institution such as WHO prequalification (WHO PQ) whose regulatory decisions and/or regulatory work products are relied upon by another regulatory authority to inform its own regulatory decisions’.
The guidelines further highlight that ‘Each NRA should define its own strategy for an appropriate risk-based approach to reliance, which includes factors such as the type and source of products evaluated, the level of resources and expertise available in the NRA, the public health needs and priorities of the country and opportunities for reliance’.
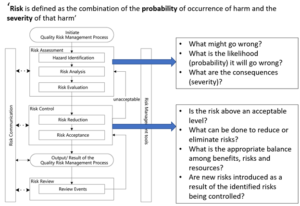
Further information on Quality Risk Management can be found in ICH Q9(R1) – 2021 and in the 2013 WHO guidelines on Quality Risk Management. The approach is summarized in the below diagram derived from ICH Q9(R1):
When identifying a reference regulatory authority, the below principles can be followed:
- It should be based on objective criteria, including evidence that the authority can be trusted (e.g. WLA, benchmarking, audit, accreditation, other information about the actions taken by an NRA), and the possibility to access the minimum required information in a language that is understood or can be easily translated.
- It should consider the capacity of the reference NRA to conduct the regulatory function independently (e.g. maturity level, or technical capacity to review further a dossier) and the capacity of the relying NRA compared to the reference regulatory authority to conduct the activities of a certain function (i.e. can the reference NRA do the assessment as well or better than the relying NRA? However, a minimum level of ML3/4 or WLA should be expected)
- It should be specific to one particular type of products and regulatory function (e.g. an authority may be ML3 for vaccines but not for medicines, or ML4 for vigilance but ML1 for marketing authorizations)
- It should be reconsidered regularly based on experience (e.g. for Marketing Authorizations, considering the frequency of substandard and falsified products).
- As a best practice, the relying NRA when applying reliance, should at least verify sameness. A checklist and guidance to conduct verification of product sameness for NRAs to use as reference can be found in the Appendix 2 of the 53rd report of the WHO Expert Committee on Specifications for Pharmaceutical Preparations (page 259) for Marketing Authorizations and Regulatory Inspections)
- It is recommended to publish on the NRA website a guideline on reliance, which defines the scope, criteria and principles followed to select reference authorities and how such assessment will be used, together with information which may be updated more regularly on which are the accepted reference regulatory authorities (for one particular type of product/function or type of decision). This will help stakeholders to comply with the NRA’s expectations.
Minimum information required for reliance
The below document was developed to support the implementation of this strategy. There would be 2 main usages of this information:
- Recommendations to guide relying countries on what is required as a minimum for them to be able to rely on other organizations.
- Recommendations to SEARN countries on what to publish/make available (in relation with AP3 information sharing and AP4 internal platform) in order to facilitate reliance from other countries on their own decisions.
Acknowledging that the implementation of these recommendations may require addressing practical and technical challenges, and in some cases further discussions and agreement of other authorities, the adoption by the Assembly of SEARN will be followed by an implementation period of two years.
The information identified in the below table intends to present the minimum information required for reliance. For reliance, the ultimate requirement is that the relying NRA should have sufficient trust in the reference authority to use the output of their work in their own regulatory decision-making system. Abridged assessment may require additional information.